
De dónde viene el término «Sistema» en el TID. Referencias
El TID ha sido visibilizado gracias a los esfuerzos de las personas que lo viven, dentro y fuera de redes sociales. Una duda común es sobre el término «sistema». ¿De dónde surgió? Hay quienes creen que fue inventado por Tumblr, y más recientemente, se dice que fue inventado en TikTok.
Pero en realidad es un término clínico que se ha usado desde antes del internet, y surge de mucho tiempo antes.
Vamos a revisar el uso del término «sistema».
Nos dimos a la tarea educativa de encontrar en nuestro material físico y digital sobre trauma y disociación referencias del uso de la palabra sistema en referencia al conjunto de identidades (alters /estados /personalidades/ partes) disociadas en una persona con TID.
Los hemos encontrado con estos términos:
- Personality system
- System of personalities/ alters / selves
- Self-System (sistema del Yo/Self)
- Internal / inner system (sistema interno)
- Multiple system
- Dissociative system
- MPD/DID system
- Ego-state system (sistema de estados del ego/yo)
- System parts (partes del sistema, sistema de partes)
- Identity system
Nota. Muchos textos tienen muchas citas, así que solo ponemos algunos y no todos por texto.
Referencias encontradas:
—1
Recognizing that (1) alters vary in their complexity and elaboration, and (2) different persons’ systems or complexes of alters have different styles of operation.
…
Yet DID patients often will acknowledge that their personality systems are actively switching and/ or far more active than it would appear on the surface (Loewenstein et al., 1987).
…
I am allowing myself to hope that Mariska’s personality system and, therefore, she, will be more readily accessible than in most DID patients.
Paul F. Dell. (2009) Dissociation and the Dissociative Disorders (p. 609). Taylor and Francis. Kindle Edition.
—2
First, thanks to Mazey, the ageless brown-skinned guardian of our system, for all the guidance and love she’s given me in my quest for recovery and wholeness. Countless times Mazey held the system together when I was no longer able.
…
While my outside world has been lonely and empty, relationships developed among some of my parts, forming a «system» of alter personalities. Each new painful experience created new parts more real than the people | knew outside of me. Personalities were forced into being — some exploded into my life. Each has a name and specific job, and some have missions. Having a reason for existing is how we cope.
—3
• Dissociation is a creative way of keeping the unacceptable out of sight. • It is a way for the DID internal system to protect secrets and continually learn to adapt to the environment.
…
Also, the dissociative personality system is usually set up to avoid detection.
…
Alters who are in place to protect the system are going to be very careful about not letting the therapist get too close initially.
Haddock, Deborah Bray. (2001) The Dissociative Identity Disorder Sourcebook (Sourcebooks) . McGraw-Hill Education. Kindle Edition. (p. 83) 2001
—4
Keep the whole system in mind. When we explore the internal system of parts, we must think of the whole picture and try to include all parts and voices.
Mosquera, D. (2020b). Voces y partes disociativas: Un abordaje práctico basado en el trauma.
—5
Example: A cis gendered female was sexually abused as a child. A male part of her was dominant and “knew” he was not abused because he was male. The dominant male part got gender reassignment cleared by their therapist. In further therapy, DID was diagnosed, and as the system of parts was worked with, it became clear to the client that they belonged in a female body.
…
Step 6: Integration and reconfiguration of the system. As parts are worked with and unburdened, the system of parts may become reconfigured.
…
Concrete thought processes: In trance people are very concrete. In addition, most child parts have childlike vocabulary. It is best to communicate clearly and concretely and to use vocabulary that the whole system will understand.
Twombly, J. (2022). Trauma and dissociation informed internal family systems: How to Successfully Treat C-PTSD, and Dissociative Disorders.
—6
Por ejemplo, una paciente con TID presentaba una alta impulsividad que se manifestaba en una conducta autodestructiva, que en realidad se relacionaba con la activación de una PE de la personalidad. Cuando trabajamos con el sistema interno de partes disociativas, este síntoma desapareció. Después de esto, la paciente no presentó más reacciones impulsivas.
…
Estas partes tenían todas ellas una perspectiva de primera persona muy elaborada. A lo largo de la terapia se hizo evidente un sistema interno de partes disociativas muy complejo y muchos síntomas borderline se pudieron explicar como manifestaciones de su TID.
Mosquera, D. (2014). Borderline Personality Disorder and EMDR therapy.
—7
Paso 1
Se nombran y describen las partes que conforman el sistema interno para que todas sean identiicadas y poder así empezar a trabajar con cada una de ellas. El terapeuta debería reconocer y respetar el significado que la paciente le da al TA, cómo funciona la disociación como defensa y cómo el cliente puede cumplir las demandas de las partes intentando evitar el conlicto interior.
Seijó, Natalia (2015). Trastornos alimentarios y disociación. ESTD Newsletter, 4 (1).
—8
Al pasar el tiempo, ir acumulando más experiencias negativativas y sentirse rechazadas por el resto del sistema, acaban funcionando como persecutorias. El paciente describe sintomáticamente esto como fenómenos de influencia (siente que una parte de él o algo ajeno a él le impone pensamientos, sentimientos o acciones), alucinaciones o pensamientos obsesivos.
…
Si esta introyección corresponde a un abusador, acabará constituyendo una parte persecutoria en el sistema. A veces el paciente llega a estar realmente convencido de que esa parte de su mente es realmente el abusador.
…
Se refuerza aquí la función protectora de esta parte que la asusta, tratando de ayudar a la paciente a entender mejor la estructura de su sistema interno.
Anabel González; Dolores Mosquera. (2015) Trastorno de identidad disociativo o personalidad múltiple (Psicología) (Spanish Edition) (p. 100)
—9
Often referred to as alternate personalities, these are the internal members of the MPD system. Changes between these personalities, or states of consciousness, are described as switching.
…
Q) Am I different than I was before the diagnosis? Are weird things going to start happening around me?
A) You, as a system, are not different. You, as a group, have lived, survived and functioned for virtually your whole life. This diagnosis makes you feel differently about yourself, but you haven’t changed. You may choose to change your lifestyle/habits/friends, etc., but your life won’t change of its own volition. You are what you have always been.…
I wish I’d known that it would be so difficult to unscramble our complex system and that there could be so many fragments that need to be “discovered” to complete the person that I am. —Jo Anne M.
…
The ISH is the strongest protector of the system, yet most understand the healing nature of painful abreaction and so allow it to happen for the long-term goal of health. The therapist would do well to listen closely to his or her suggestions.
…
Being a good role model will teach a multiple to parent his or her own system. This is a priceless gift.
…
What she will look like, I do not know. But I know many of the personalities that make up her system of alters. I have made friends with them, and I feel they trust me. I do not like what some of them have done to her, but I think I understand why they had to do it.
…
Contracts. Verbal or written agreements made between therapist and client for the express purposes of serting safe and reasonable boundaries for the client, to nurture the client’s sense of cause and effect, and to encourage the internal system to take responsibility for its behavior.
…
Inner self-helper (ISH). An alter among the typical group of helper or protector personalities. Therapists have found ISHs present in the majority of individuals diagnosed with MPD. Generally, an ISH has complete information and a good understanding of the workings of the system.
…
System. The structure of relationships within the internal world of an individual who has MPD… It is often helpful for a person with MPD to make a map or diragram of his/her internal personality system
M. Cohen, Barry. Giller, Esther. W. Lynn et al. Multiple Personality Disorder from the Inside Out. (1993) (p. 228)
—10
…have them help heal the distressed parts, and bring choice and conscious control to the whole of each client’s system.
Shapiro, Robin. Easy Ego State Interventions. Strategies for working with parts. (p. 29) (2016)
—11
This expert said that he was «unable to render further opinions regarding the remainder of the defendant’s personality system, particularly the host personality, because there is simply no scientifically acceptable way to assess the mental state of alter personalities who were not co-conscious at the time of the crime» (p. 350).
…
I feel it is important to acknowledge the limitations of psychotherapy. A little bit of help can be provided in relation to facilitating communication, thought, and collaboration between different parts of a dissociative personality system, strategies of affect regulation can be taught, and a general ambience of support and respect can be offered.
—12
These ‘alter’ personalities can assume almost any identity since they seem to be constructed on the ‘logic’ of dream or trance, in which anything is possible. Thus, alters may be male or female, adult or children, human or non-human. Quasi-spiritual entities are not uncommon. Usually, but not always, there is one personality which the system as a whole regards as the main identity which is presented to others..Often different personalities are created for particular roles – eg. going to work, being sociable, being sexual etc. Traumatised children are also commonly found. These may be guarded by special protector personalities, who may be hostile to the therapist if the children are perceived as in danger. The degree of awareness of the overall system varies amongst the personalities, some having very limited awareness and others having considerable overview.
…
Despite the radical alteration of the sructure of self-experience in MPD/DID, it should not be assumed that this is like a smashed or shattered state of mind, as found sometimes in more simple instances of PTSD. The multiple system of personality is highly organised, each part carrying out particular functions and having relationships to one another, as in any complex organisation.
…
Psychotherapy with a multiple personality system will destabilise that system through the very fact of its existence being diclosed – such systems are intended to be secret.
Mollon, Phil. (2011). Dark Dimensions of Multiplicity (pre-publication version) In: V.Sinason (Ed.) Attachment, Trauma, and Multiplicity. Routledge. London. 2002/2011.
—13
The therapist comes to better appreciate the unique issues and perspectives of the personalities, and to understand how the alter system responds to particular issues or stressors. With this knowledge, the therapist uses the tools established in stages 1 and 2 to address problems experienced by particular alters and in the function of the system, and presses for still more cooperation and collaboration. Many experts (16,18) feel that it is dangerous to progress into work on traumatic material without first getting “the lay of the land,” and being able to anticipate how the system will react to dealing with traumata.
…
Most DID patients are treated in therapies that have a psychodynamic or cognitive-behavioral orientation, and are facilitated by additional modalities and approaches. An addition to conventional approaches is “talking through” (45, 46), that is, talking to the personality system as a whole. In this manner the therapist keeps in mind that any and all parts of the mind may be listening, and by appealing to all parts of the mind, one encourages as many to listen as is safe and/or relevant. Also, the therapist develops a pattern of talking to both the individual alter or alters with whom the therapist is in conversation, and the person as a system and as a whole, at the same time.
Kluft, R. P. (1999). An Overview of the Psychotherapy of Dissociative Identity Disorder. American Journal of Psychotherapy, 53(3), 289–319. doi:10.1176/appi.psychotherapy.19
—14
In Chapter 11, Safety and Welcome: The Experience of Earned Secure Attachment, we address “integration” not as a goal of treatment but as a process that occurs organically when we use mindfulness-based techniques to bring awareness and compassion to the system of traumatized parts. As defined by Daniel Siegel (2010), “Integration results from differentiation coupled with linkage.”
…
Just as each individual responds to trauma differently, we would expect each client’s structurally dissociated personality system to be unique.
…
The «decoding» of parts activity outside the normal life self’s consciousness is an extremely important focus of DID treatment that should never be conducted judgmentally, without empathy for the parts in question. And it helps the client become familiar with his or her own system –
Fisher, Janina. Healing the Fragmented Selves of Trauma Survivors. Overcoming Internal Self-Alienation. (2017) (p. 26)
—15
Entonces, en lugar de verme a mí misma como loca o defectuosa, podía considerarme como fuerte e inteligente. Mi extraordinario sistema de partes me había ayudado a desarrollarme como persona, a tener amistades y a destacarme en la escuela y en los deportes.
Trujillo, Olga R. La Suma de mis partes. Testimonio de una sobreviviente de trastorno de identidad disociativa. (p. 221) (2019)
—16
Again, traumatized inner systems are delicate ecologies. Just like with external ecologies, changes in one aspect can have unforeseen consequences. This is far less likely, however, if you think in terms of systems—then the consequences often can be foreseen and preempted or dealt with from Self.
Of course, this map doesn’t just apply to inner systems. It has been used effectively to understand and work with families and corporations, and I believe it applies to human systems at any level. Systems of parts and people tend to polarize, form protective alliances, and exclude or cut off from each other whenever they are traumatized and lack effective leadership.
…
I learned many years ago the importance of respecting protectors and their right to protect the system and to not be pushed out of the way. Burdened inner systems are sensitive environments and we need to approach and visit them accordingly. Your protectors have spent a lifetime trying to keep you (and everyone else) away from your exiles, so they need to be consulted first and convinced that there is a good reason to let you go there. We don’t go to exiles without permission from protectors.
—17
Most people now being diagnosed with MPD have a number of alters, rather than just one, which are combined in what is conventionally called a ‘system’. There are endless variations: some make angry, aggressive alters to protect the children, or friends to alleviate loneliness, or torturers who mimic abusers. Some people have only child alters, but others go on making new personalities, which may be any age. Most MPD systems contain at least one member of the opposite sex. Some include animals.
Usually at least one member in a system is in some way disruptive, and the behavior of alters—promiscuity, self-harm, addiction, aggression, phobias—is often what first brings people with MPD to the attention of a therapist. However, the crucial thing about the disorder, which distinguishes it from normal multiplicity, is not the nature and behavior of the alters but the fact that they do not share a common memory. Although some personalities may share information there is always a communication gap in an MPD system. The normal household, as multiple systems are sometimes called, is open-plan, while in people with MPD, at least some of the personalities live in watertight compartments.
Carter, R. (2008). Multiplicity: the new science of personality, identity, and the self. Little Brown and Company
—18
La manera en que llevamos a cabo nuestra entrevista, comprobando cómo se encuentran las partes y manteniendo en mente el sistema como un todo, ya es en sí misma una intervención integradora.
…
Sistema interno
Este término hace referencia a la representación mental que se hace el paciente “cuya estructura mental está fragmentada” del conjunto de los diversos aspectos o partes de su propia mente. El sistema interno incluye partes disociativas, recuerdos, emociones y cualquier otro aspecto disociado de la persona. Entender las partes como un sistema más que como estados de la personalidad por separado aporta un importante marco de referencia para el tratamiento. El capítulo 4 explica en detalle cómo explorar el sistema interno.
…
Sin embargo, la mayoría de los pacientes que escuchan voces o tienen sistemas internos complejos no están preparados para este procesamiento al principio de la terapia y necesitan una preparación adecuada. Para determinar si es seguro para el paciente procesar el trauma con procedimientos estándar, deberían darse, como mínimo, las siguientes condiciones:
• Conocimiento suficiente del sistema de partes.
• Información adaptativa. Sin información adaptativa el paciente no está preparado para integrar ningún trabajo de trauma.
• Cierta capacidad de autorregulación o la capacidad de regularse con el terapeuta (corregulación).
• Capacidad de mantener la atención dual, incluso aunque solo sea posible con ayuda del terapeuta.
• Capacidad de notar el cuerpo y tolerar las sensaciones físicas.
• Coconsciencia entre partes disociativas o haber alcanzado acuerdosen el sistema.
• Cierta contención fuera de la terapia. El apoyo social es ideal, pero si no lo hay, por lo menos ser capaz de pedir ayuda.…
El lugar de reuniones
El procedimiento del lugar de reuniones (González, Mosquera y Solomon, 2012) se desarrolló a partir de técnicas para explorar el sistema ya existentes como la terapia de grupo interna (Caul, 1984), la técnica de la mesa disociativa (Fraser, 1991, 1998) y la sala de reuniones (Paulsen, 1995, 2009).
…
Como último paso, es importante que el sistema llegue a acuerdos o compromisos que todas las voces y partes puedan aceptar en beneficio de todo el sistema.
…
El cierre de Ja sesión es posiblemente uno de los momentos más relevantes del trabajo. Es importante no terminar de manera brusca, sin tomarse el tiempo suficiente para explorar cómo se encuentran tanto el paciente como el sistema. Muchos pacientes parecen estar bien, pero hemos de recordar que esto es una estrategia aprendida.
Mosquera, D. (2020). Voces y partes disociativas: Un abordaje práctico basado en el trauma.
—19
Parts that are «out» may be entirely unaware of the other parts of the system.
…
The first step in this collaboration is to assure the internal system that all parts are welcome and that all of them – even those who are suicidal or destructive – were formed in an attempt the self-system, no matter how much they now seem to threaten it.
Van Der Kolk, Bessel. The Body Keeps the Score. Brain, Mind, and Body in the Healing of Trauma. (p.284-285) (2014)
—20
Los terapeutas que han sido formados para ver a los demás como seres humanos complejos con múltiples características y potencialidades pueden ayudarles a explorar su sistema de partes internas y cuidar las facetas heridas de sí mismos.
…
Las partes que están «fuera» pueden ser totalmente desconocedoras de las otras partes del sistema.
…
El primer paso en esta colaboración es asegurar al sistema interno que todas las partes son bienvenidas y que todas ellas (incluso las que son suicidas o destructivas) se formaron en un intento por proteger al sistema del yo, por mucho que ahora parezcan amenazarlo.
Van Der Kolk, B. (2020). El cuerpo lleva la cuenta: Cerebro, mente y cuerpo en la superación del trauma. Eleftheria.
—21
Switch is eight years old. He held incredible rage for being abused, but he also felt a powerful allegiance to one of our abusers and turned that rage toward me and some of the others. Switch harmed my body many times. He is not so angry anymore, and he has been accepted by everyone in the system. Switch has his own sheriff’s badge now, which he likes to wear around. He is a member of the core group.
…
Arly folded her hands. “It’s a long haul,” she said, “but people do recover from this. In some cases, eventually there’s a full integration of all of the personalities into one, and in other cases, where the personalities prefer to stay separate, they can work toward achieving cooperation so the whole system can function relatively smoothly in the world. Either way, like I said, it’s a long haul.”
—22
The personality system of patients with classic forms of MPD would generally include relatively more substantial personalities and fewer personality states, while patients with subtle forms would usually have more personality states and fewer personalities, or perhaps only personality states. Some multiples with subtle forms could be complex multiples with 26 or more personalities and personality states (Kluft, 1988) or polyfragmented multiples (Braun, 1986).
…
A case of multiple personality whose personality system was basically covert and subtle will be presented, and excerpts from her therapy will be used to illustrate the subtle signs of dissociation and other dissociative symptoms observed in MPD patients.
Franklin, J. (1988). Diagnosis of covert and subtle forms of multiple personality disorder through dissociative signs. Dissociation: Progress in the Dissociative Disorders, 1(2), 27–33.
—23
For me, the point of therapy is for our clients to become happy, functional, and relatable people. The point of ego state therapy is to find internal resources, bring them to the front of consciousness, enhance them, have them help heal the distressed parts, and bring choice and conscious control to the whole of each client’s system.
Shapiro, R. (2016). Easy ego state interventions: Strategies for working with parts. W W Norton & Co.
—24
Sorpresivamente, no me habló de sus hermanas «reales», sino de 4 hermanas que constituían su sistema interno de partes disociativas. De esas cuatro, hasta el momento solo me había hablado de una.
…
Este es un punto crítico en el desarrollo del tratamiento. Si el terapeuta no se siente cómodo con la idea y el concepto de partes disociativas, probablemente tampoco se sienta cómodo con ninguna de las estrategias utilizadas para trabajar con todo el sistema interno. Esto puede llevar a un tratamiento ineficaz dado que mucha de la sintomatología disociativa seguirá estando presente por no haber sido adecuadamente tratada
…
Una vez que se han identificado las partes disociativas es recomendable que el terapeuta realice lo que se conoce como mapeo del sistema (Putnam, 1989)
Baita, Sandra. Rompecabezas. Una guía introductoria al trauma y la disociación en la infancia. (p.222) (2015)
—25
In this drawing, Dalma showed her complete internal dissociative system to me. She said, “Nada is really angry, she’s mad at Daddy, she doesn’t want to take a bath with him. Mary is the older one, she’s older like a grandma, she’s 89, Lily is the best, she’s really good, not like Nada, she’s the worst. Daddy used to touch Debora’s private parts in a room, and Dalma saw this, Beatriz too.” As she referred to Dalma in the third person, I assumed that there might be another part talking, so I asked who was the one talking? She skipped the question and kept saying: “Debora said, ‘Please don’t do this anymore,’ and Daddy would say ‘I won’t, I promise, can you forgive me?’ And Debora always forgave him.”
…
The most important thing for the clinician to understand is that, without an adequate identification of the personality system (Silberg, 1998), you will only work partially, with only one aspect (feeling, memory, sensation) of the whole experience, and you will not be able to progress into any trauma resolution.
Wieland, S. (2015). Dissociation in Traumatized Children and Adolescents: Theory and Clinical Interventions: Second Edition. 10.4324/9781315740430.
—26
Smith paused for a second. «Think about it. The whole system was set up very early, probably between ages one and four, back during Baby’s years. The terrible abuse gave rise to Bobby as naughty boy, Tommy as bully, and the Witch as apologist.
…
I don’t just mean the terrible things that Tommy does to Bobby. Your whole internal system thrives on hate and guilt. Every one of you is caught up in a cycle that must be broken.»
…
Perhaps because we were speaking about a single topic, searching for a coherent conclusion, our deliberations seemed more organized. That was remarkably new in an MPD system that had always been as fragmented and fractious in its conversations as in its personalities.
Oxnam, Robert. B. A Fractured Mind. My life with multiple personality Disorder. (2006)
—27
Como la paciente no elabora ninguna respuesta ni varía su estado, intento establecer alguna comunicación con el sistema interno. Habíamos usado este procedimiento otras veces con buenos resultados, pero en este momento tampoco parece funcionar.
T: ¿Entiende el Hombre de Negro lo que estoy diciendo? ¿El se da cuenta de que es diferente de aquel hombre?
…
Cuando trabajamos en el contexto de mucha fragmentación, con partes con mucha autonomía, la intervención ha de graduarse al milímetro y el paciente y el sistema interno de partes han de ir tomando la decisión a cada paso. Esto no solo permite ajustar la dosis de EB a introducir, sino que ayuda a que el paciente se sienta respetado y partícipe del proceso.
…
Por supuesto, teníamos que consultar con el sistema interno. Aunque con el dibujo esta parte disociativa no se desvelaba, la comunicación con ella de modo más indirecto era fluida.
T: Haz la pregunta al interior, como siempre, de si está de acuerdo en trabajar con la dificultad para mirar el círculo.
P (cerrando los ojos): Dice que «sí, pero poco».
—28
Dissociation is an oddly invisible defense since when one alter or system of alters is running things smoothly, therapists do not see the dissociative process in operation and may therefore believe they have never seen a dissociative patient (McWilliams, 1994).
…
EXTENT OF THE DISSOCIATIVE SYSTEM
Multiplicity exists on a continuum, and according to Kluft (1988b) the degree of multiplicity experienced by any one individual depends on the amount and severity of the trauma, the degree of dysfunction, the amount and quality of the internal communication among part-selves, and the degree to which the different alters or «parts» cooperate. Networks of alter personalities can vary greatly in their size, their permeability, and in the way aggression is distributed among them to serve developmental functions, trauma containment, and the self-hatred that keeps much of the system running.
Trie degree of overtness of the alter phenomenology may depend, according to Kluft (1996a), on the resilience of the host alter, the incidence of contemporary stress in the patient’s life, the influence of secondary gain, the evidence of narcissistic investment in separateness, and the extent of underlying cooperation and number of shared goals within the dissociative self-system.
…
Many patients speak of radical splits in their dissociative identity systems between «day» selves and «night» selves and insist on keeping these separate long after their involvement in perpetrator groups has ended.
Schwartz, H. L. (2000). Dialogues with Forgotten Voices : Relational perspectives on child abuse trauma and treatment of dissociative disorders.
—29
DID patients are among the most disturbed people who seek the services of mental health professionals, yet they are often among the most treatable. The treatment must be guided by an understanding of DID and its historical antecedents. The complex details of the personality system can overwhelm the therapist who doesn’t have a broad framework within which to conduct therapy.
…
The self-destructive behavior is not usually primarily a “cry for help” or “attention-seeking,” and is most often a sign of internal dispute, cognitive errors, and hostility in the personality system.
…
The first problem in treating DID is how to think about the personality system. Some of the resistance to the diagnosis is due to nomenclature. What are we saying when we say that a patient has a number of different personalities inside her?
Ross, C. A. (1997). Dissociative Identity Disorder: Diagnosis, Clinical Features, and Treatment of Multiple Personality. Wiley-Interscience.
—30
Moreover, as I mentioned earlier, when management of the personality system is not under control, the multiple may make numerous inopportune and time-consuming changes of dress within the course of a day, even among personalities of the same sex.
…
Second, integration may involve only some of the personalities within the total system of alters. Partial integrations, however, are often a first step toward total integration, and when either sort of integration occurs, characteristics seem to blend and reorganize rather than disappear.
…
One might think that the presenting personality should be considered primary. But that alter often turns out to be relatively recent and fairly peripheral in the multiple’s total system of alters.
Braude, S. E. (1993). First person plural: multiple personality and the philosophy of mind. The Philosophical Quarterly, 43(171), 272. https://doi.org/10.2307/2220390
—31
Related studies, based on the analysis of case reports, clearly indicate that information acquired while one personality is in executive control of the body is still available to the system, although it may not be consciously accessible to other personalities at a given point in time (13, 20).
…
However, multiple personality disorder patients who were victims of child abuse always have some form of sexuality present in their system of personalities. Another difference between these two groups concerns the ability to experience joy or pleasure. Nonmultiple personality disorder child abuse victims are fre- quently anhedonic. In contrast, child abuse victims who devel- oped multiple personality disorder are still able to experience happiness and pleasure in their ongoing lives. These capacities are preserved by some personalities.
Kluft, R. P. (1985). Childhood antecedents of multiple personality. American Psychiatric Pub.
—32
THE PERSONALITY SYSTEM
The alter personalities are fascinating, and the differences amon.g them can be distinct and dramatic. It is important, however, always to remain aware of the patient as a whole person. The »personality» of an MPD patient is the sum and synergy of the system of alter personalities.
…
Mapping the personality system
The idea of mapping the personality system of MPD patients is not new; both Morton Prince (1909a) and Walter Franklin Prince (1917) published diagrams of their understanding of how alter personalities of their patients fit together. Bennet Braun (1986) has expanded the idea of mapping into a useful therapeutic technique.
…
The form of the map also provides information about the personality system’s internal metaphor, which can be used in working with the system.
Putnam, F. W. (1989). Diagnosis and treatment of multiple personality disorder. Guilford Press.
—33
Como ya hemos indicado anteriormente, la personalidad de todo el mundo es un sistema dinámico complejo que, como todos los sistemas, conlleva continuas acciones y reacciones, en las que partes de dicho sistema interactúan para mejor o para peor.
Boon, Suzette/Steele, Kathy/Van der Hart, Onno. (2014) Vivir con disociación traumática (Biblioteca de Psicología) (Spanish Edition) . Dessclée De Brouwer. (p. 56)
—34
SYSTEM pictures depict an array of individual elements forming and working as a unit that represents the current internal organization of parts-selves.
…
The therapist working with MPD must always work within the system of alter personalities to effect change. «System» refers to the interrelation among alter personalities and other parts who inhabit the inner world of the MPD client and who usually function on her behalf. Just as any organization, members may work well together at certain points in time, and not at others.
Cohen, Barry M. Thayer Cox, Carol. Telling Without Talking. Art as a window into the world of multiple personality. (p. 21) (1995)
—35
Systems can have any number of alter personalities, from two to a great many. Generally, it is believed that the earlier the trauma occurs, the more extreme the trauma is, and the longer time during which it occurs directly bear upon the number of resulting parts. The kind and amount of support one receives at the time of the trauma, as well as afterward, can also make a difference.
…
The System Map is like an internal family tree, though it can be drawn out in whatever format, in whatever way is easy for the System to understand. It will contain and illustrate information such as who split off from whom and how you all relate to each other. As you become more aware of your System over time, your System Map may grow as you encounter newly discovered parts.
A.T.W.. Got Parts? An Insider’s Guide to Managing Life Successfully with Dissociative Identity Disorder (New Horizons in Therapy Book 1) . Modern History Press. (2005)
—36
My studies over the years have taken me into systems and what makes organisations function in the way they do. Individuals in organisations sometimes can’t recognise what happens when it is far removed from their own position. Systems reflect the pressures that come from inside as has been well documented by Obholzer et al. (1994). There is a system within the person and a system that the person lives within. The total system is the whole of society, but people exist within microsystems, sometimes family, sometimes support services and, of course, for people with DID, often within a cult. The power of systems should not be underestimated. Ritualised abuse can produce systems with internal destructive systems as well as the fractured personality that enables power to be retained by the abusers. The systems within systems are confusing and exhausting for the individual affected and for those who support them. It is common for people with DID to refer to their body and their internal system as separate entities, making statements like “the body’s age is …” and “within my system there are many alters, all with their own role”. It is a joy to meet people with DID who have found a way to live a good life and some of them have written chapters in this book.
The internal system of someone with DID is fragmented and only has some communication lines on the inside.
…
A few months ago we started another course, a diploma in horticultural studies. A far cry from literature perhaps, but more in line with my system as a whole. One of my little ones loves gardening, and although she is not old enough to attend the classes, she feels respected by the fact it is an area that she is interested in and can, in her own way, relate to. This means she is more supportive of the system attending, and does not need particular resourcing in order to do so. It is also academically at a level that means that several of my older alters can actively participate. It is more in tune with where we are as a system at the moment.
Bowlby, X., & Briggs, D. (2014). Living with the reality of dissociative identity disorder: Campaigning Voices. Routledge.
—37
Although they may be harder to understand, these latter ego states are often the protectors of the system, because protecting the system, which seems ludicrous to an outsider, gives consistency to their inner world.
Hunter, Marlene E. Understanding Dissociative Disorders: A Guide for Family Physicians and Healthcare Workers. (2009) (p. 14)
—38
Advocacy and apology. A small but vocal minority of MPD .patients are vehemently opposed to any change in their system of alters. Some perceive the alters as real people, and they are appalled at any attempt to reason to the contrary and »do away» with members of their inner families (see Chase 1987).
…
The goal is not to achieve a fusion – any results will be transient. Instead, it changes the characteristics of the alter system for a brief period of time, during which the patient may become more accessible to other interventions.
…
A Fifth pathway might be termed a «brokered departure». In such cases, an alter’s ceasing to be separate is virtually negotiated within the alter system. Such alters may report or be reported to have joined with one or several alters in a planful way.
Kluft, Richard P, M.D., Fine, Catherine G., Ph.D. Clinical Perspectives on Multiple Personality Disorder. (p. 121) (1993)
—39
El terapeuta que se acerca a sus primeros casos de TID corre el peligro de pasar a ser un elemento más del sistema de partes del paciente, cronificándolo más que ayudando a su evolución hacia sistemas mentales más adaptativos.
…
Todo el sistema interno del paciente ha de asumir la responsabilidad. El modo en que esto es manejado por el individuo está muchas veces conectado con la responsabilidad negada o puesta en otros de las figuras relevantes en la infancia del sujeto.
…
Cuando existen barreras muy marcadas entre los estados mentales, este proceso ha de ir acompañado, de modo paralelo, de un trabajo con el sistema interno, como describíamos en el capítulo del trabajo con partes.
González, Anabel. Trastornos Disociativos. Diagnóstico y Tratamiento. Ediciones Pléyades. S.A. (2010) (p. 237)
—40
Any increase in symtoms, reduction in function, or series of crises for no apparent reason, is a red flag. What is going on? The answer could be: ongoing trauma or conflict in the present; some internal system conflict; host resistance; or the therapy going too fast.
…
In order to treat flashbacks in DID, it is essential to understand the system conflicts and dynamics that are driving them.
Ross, Colin A. M.D. Treatment of Dissociative Identity Disorder. Techniques and Strategies for Stabilization. (2018)
—41
If inner conflicts are minimized, DID alters can learn to cooperate like a well-coordinated soccer team; where all the players work together for a common goal. Each member of a soccer team has a particular position, using a specific skill set. This is directly analogous to a cooperating DID system.
…
Most of the alters were just too young for me to employ these techniques. Eventually, I found that the most appropriate approach for Joan was to just talk to the alters, and work with what arose on an ad hoc basis. I let the system decide, in its internally assessed order of urgency, who and what needed to be dealt with during each session.
Yeung, David. Engaging Multiple Personalities. Volume 1. Contextual Case Histories. (2014) Preface.
—42
In much the same way, dissociative clients can only start to talk about the untellable when the inner system is co-operating and the therapeutic environment is sufficiently contained.
George F. Rhoades, Jr. PhD. Vedat Sar. MD. Trauma and Dissociation in a Cross-Cultural Perspective (pp. 310-311) (2006) Taylor and Francis.
—43
Our system has several children (Claire 7, Miles 8, Sidney 5, Karen Boo 2, Julie 13, and Karen 1).
…
Miles–8 years old–Miles can’t trust anyone, but has developed some feelings for you, Dr. Bear. Miles was created to hold all of the anger. He doesn’t want anyone to know about the system.
Also, since Claire’s letter, Karen is becoming more aware of and familiar with her split-up internal system and I can now talk to her about it.
…
Although she feels there are other parts inside her that are more capable of talking to me, I regard Karen 3 as the person I’m talking to and treating. But I really have no basis for regarding her as any more dominant or primary than any other part in her system.
Baer, Richard. Switching Time. A Doctor’s Harrowing Story of Treating a Woman with 17 Personalities. (2007)
—44
The alter stated that she had rung up the service herself to express this and that staff had asked the host and not her to contact them. The participant described the experience as follows:
My perspective on it was that if they want to treat me, they’ve got to treat all the others as well because… if they’re saying… to some of them, “No you can’t talk,” to me that makes the whole situation worse. You’re just fighting against… the whole system. You’re not bringing them all together… I think you’ve gotta talk to the others to make that happen and if you’re only just talking to me, what’s gonna happen when I leave that hospital for treatment?… I kept thinking yeah I can just see it. They’re [alters] gonna get angry, they’re gonna start doing this, that and the other and fighting against it. What’s the point in that? (P2)
Jessica Floris & Susan McPherson (2015) Fighting the Whole System: Dissociative Identity Disorder, Labeling Theory, and Iatrogenic Doubting, Journal of Trauma & Dissociation, 16:4, 476-493, DOI: 10.1080/15299732.2014.990075
—45
Thus, a systemic approach that considers dissociative parts as interrelated psychobiological subsystems of the individual’s larger personality system should be the fundamental foundation for all therapeutic interventions.
…
When possible, the therapist “talks through” the ANP to various other parts rather than encouraging switching between them, thus working with the personality system as a whole.
Courtois, C. A., & Ford, J. D. (2013). Treating Complex Traumatic Stress Disorders (Adults): Scientific Foundations and Therapeutic Models. Guilford Publications.
—46
One might ask why a patient who utilizes the mechanisms of splitting develops the characteristics of multiple personality rather than a borderline or narcissistic personality. This question remains problematic. Greaves (1980) attempts an explanation by suggesting that «.. .. alter selves, though woefully incomplete as personality systems, may nevertheless represent a level of ego organization which is higher than that of borderline personality. It is this feature which allows the alter selves to age, acquire experience and assume additional degrees of identity.»
Weiss M, Sutton PJ, Utecht AJ. Multiple personality in a 10-year-old girl. J Am Acad Child Psychiatry. 1985 Jul;24(4):495-501. doi: 10.1016/s0002-7138(09)60571-9. PMID: 4019981.
—47
Este enfoque permite a los estados de ego tener un verdadero cambio con el terapeuta. Durante el tratamiento, se estimula a cada estado a contar sus propias experiencias dentro del sistema, y se le reconoce su participación.
…
Los estados de ego infantiles en un adulto son peligros potenciales inminentes. Para lidiar con ellos es conveniente designar, dentro del sistema de estados de ego, un cuidador para estas partes jóvenes del conjunto de la personalidad.
…
Llegar a conocer a estos estados de ego no es tan difícil como parece. Lo más importante es el tratamiento respetuoso. A medida que nos van conociendo, ellos empiezan a darse a conocer, especialmente si simplemente les pedimos, respetuosamente, que se presenten y se identifiquen. Sin embargo, esto puede llegar a tomar muchos meses, y a veces años, antes de que lleguemos a conocer todo el sistema (y ellos aprendan a conocerlo por sí mismos también).
…
La resolución significa que cada estado de ego conozca a los demás, que no queden secretos entre ellos, que no haya más sabotaje interno y/o autodaño y que todas las decisiones las tomen los adultos del sistema.
Hunter. E. Marlene. MD. FCFP(C) Canadá. (2013) Manual Médico Para el Personal Cubano de La Salud Sobre Trastornos Disociativos
—48
System. This is the word we use to refer to all of the different personalities in a person with DID. This includes the one who lives out front in the world, the ones who only come out sometimes, and the ones who never come out and only live inside.
…
ACTIVITY 5.1: MEETING THOSE IN YOUR SYSTEM
Although it may take you a while before you know all of those inside you, it’s helpful to keep track of those you do have aware ness of. In activity 4.3, you generated a list of each of your alters.
Alderman, Tracy. Ph.D. Marshall, Karen, L.C.S.W. Amongst Ourselves. A Self-Help Guide to Living with Dissociative Identity Disorder. (1998) (p. 13)
—49
The alters keep the memory and act out the related emotion. At first, the alters seem so different from one another, but when we examine more closely their purposes and functions within the multiple’s system, we see that alters are interrelated.
…
The name is symbolic for the role of an alter within the multiple family system (e.g., Director was a helper personality who got everything organized and off the ground).
…
Each patient with MPD is absolutely unique. Her background, her level of abuse, the number of personalities in her alter system, the age that she experienced abuses, the level of safety and security in her present life, and other predisposing factors will affect the course and time of treatment.
—50
In this textbook he emphasized a treatment that involves intensive interaction with all the alters in a personality system. (Refiriéndose a Frank Putnam)
Hacking, Ian. Rewriting the Soul. Multiple personality and the sciences of memory. (p. 18) (1995)
—51
Se trata de una forma creativa de mantener aquello que es inaceptable fuera de la conciencia. Ayuda el sistema disociativo (TDI) a proteger sus secretos y adaptarse continuamente al medio ambiente.
Carvalho, Esly. Ph.D. Sanando la Pandilla que Vive Adentro: Como el EMDR puede sanar nuestros roles internos (Spanish Edition) (p. 35). Unknown. Kindle Edition. 2012.
—52
The alter Chrissy needed to learn boundaries. Based on Christine’s presentation in therapy, I identified her as the primary personality and kept that position throughout our work with her “system.”
Pattillo, Christine. I Am WE: My Life with Multiple Personalities. Christine Pattillo LLC. Kindle Edition. (2014)
—53
Internal Family Systems (IFS) therapy is a synthesis of two paradigms: the plural mind, or the idea that we all contain many different parts, and systems thinking. With the view that intrapsychic processes constitute a system, IFS invites therapists to relate to every level of the human system— the intrapsychic, familial, communal, cultural, and social—with ecologically sensitive concepts and methods that focus on understanding and respecting the network of relationships among members.
Schwartz, R. C., & Sweezy, M. (2019). Internal Family Systems Therapy, Second edition. Guilford Publications.
—54
While in severe DDNOS children a sense of self (or other) may be quite underdeveloped, DID children learn to compartmentalize feelings and experiences in order to survive chronic abuse and preserve a sense of self. For some children the path to dissociative identity disorder includes a period of DDNOS; a more organized system of personalities may crystallize in the teen years with the impetus to resolve teenage developmental conflicts (Hornstein, 1994) and to formulate a self-identity (Erikson, 1950). However, even very young children may have clearly defined DID.
…
Fear and anxiety may cloud the child’s memory of a previous disclosure or block verbalization of information disclosed by one part in a child’s personality system. Due to state-dependent learning, information stored or retrieved in certain settings may not be available to the child in other settings (Putnam, 1991b).
…
Many children, especially very young ones ( under age five ), may not have fully developed DID or fully formed personalities. Some may have what Fagan and McMahon ( 1984 ) call “incipient” multiple personality disorder or DID “in progress.” In those cases, there may be no need to delineate the parts and work on building communication to the extent described in this chapter. However, these techniques have worked well with the DID children I have seen in my office, who have ranged in age from six to fifteen. I find that children with DID usually have less rigid amnestic barriers between parts than adult clients and often find it easier to build awareness and communication within the system.
…
The therapist can begin to see the roles the child’s various parts play within the inner system and the roles some play (or used to play) in the outside world. Children often choose names or descriptive attributes for various parts of themselves through identification with television characters or comic book heroes, etc. This makes sense if we realize that imagining he is someone or somewhere else or has incredible powers may be the helpless child’s only sure defense against abuse.
—55
Advocacy and apology. A small but vocal minority of MPD .patients are vehemently opposed to any change in their system of alters. Some perceive the alters as real people, and they are appalled at any attempt to reason to the contrary and »do away» with members of their inner families (see Chase 1987).
…
When alters share a degree of mutual awareness of one another, they may understand themselves to have all manner of relationships with one another. For example, certain parts often care for or try to protect scared child parts. In addition, life experiences may be recapitulated in the alter system; for example, an alter based on an abuser may see itself entitled to hurt alters based on the patient’s experiences of being unable to prevent or interrupt victimization by the abuser or abusers.
The alter system frequently replicates the DID patient’s experience of the relationships and circumstances that prevailed in his or her family of origin. An ‘‘inner world’’ is commonly developed in which the alters interact. It is common that some alters active in the inner world may never assume executive control of the patient as the patient interacts with external others and may never manifest themselves in therapy unless they are sought out. Furthermore, events in this inner world constitute a ‘‘third reality’’ to the patient and may be experienced as just as real as events that take place in external reality.
…
Although the personality systems of some patients who have DID may be sufficiently accessible for treatment to proceed with no need to access and address individual alters, others may be organized in a way that will not allow treatment to move forward without such efforts. In my experience, the former group is much smaller than the latter, making it more appropriate to assume that such efforts may prove necessary.
…
In many if not most alter systems, the host is scorned and perceived as a ‘‘wimp,’’ a ‘‘human shield,’’ or ‘‘cannon fodder’’ by other alters. In some situations, one aspect of the host’s role is to shield a part or parts understood to be the true core or identity of the person. Any proclamation by the therapist to the effect that the host is the patient’s center and reason for being may encourage disruption rather than cooperation by other alters. It may convince them that the therapist does not understand what is going on, and is trying to impose an unwelcome and illegitimate authority on them.
Kluft RP. Dealing with alters: a pragmatic clinical perspective. Psychiatr Clin North Am. 2006 Mar;29(1):281-304, xii. doi: 10.1016/j.psc.2005.10.010. PMID: 16530598.
—56
Again, their system operated democratically despite the tension and hostility among them. Life had treated them so miserably, I guess, that they were very concerned with fairness.
…
But Lauren was too frightened to do anything, and her internal system was stalemated. She came to the next session blaming everyone from God on down for her misfortunes. I could hardly blame her.
Mayer, Robert. Through Divided Minds. Probing the mysteries of multiple personalities. -A Doctor’s Story. (1989) (p. 81)
—57
The individual mind may be regarded from this point of view as a complex system of many minds or, more strictly speaking, the psychophysiological individual may be viewed as an organization of many subordinate individuals.
…
It may again be that a dissociated system falls into the subconscious, and keeps on repeating itself in the form of independent states, but vaguely connected with the principal personality.
Boris Sidis, M.A. PhD. M.D. (Harvard) and Simon P. Goodhart, Ph.B.. (Yale) M.D. Multiple personality. An Experimental investigation into the nature of human individuality. D. Appleton and Company. 1904-1919
—58
Clinicians working with DID patients generally must hold the whole person (i.e., system of alternate identities) responsible for the behavior of any or all of the constituent identities, even in the presence of amnesia or the sense of lack of control or agency over behavior (see Radden, 1996).
…
As part of the emphasis on safety and self-management, the clinician will commonly develop “safety agreements” with the patient’s alternate identity system to provide a structure for the patient to reduce unsafe behaviors.
Journal of Trauma & Dissociation. International Society for the Study of Trauma and Dissociation. Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision. 2011
—59
In some respects Rivera also prescribes integration to oneness:
The more deeply parts of the individual connect with the therapist; the more important it is for the therapist to remember that the client is one person. As the therapist does this, the individual aspects of the system or personalties will gradually transform. They will not be stuck in rigid and repetitive patterns, and the early stages of a fluid responsive self will begin to emerge (Rivera, 1996, p. 122).
…
Rivera’s stance (p. 41 & p. 122) moves towards seeing communication and co-consciousness as a therapeutic end in itself, but still with the goal of developing a functional “I”. If the goal is functionality as “we”, two approaches are possible. Either therapy works towards a co-ordinated internal system, involving communication and co-consciousness between parts, or the possibility could be explored that functionality can be gained without all parts of the system becoming aware of other parts and able to communicate with them. In Bromberg’s (1993) view “Health is not integration. Health is the ability to stand in the spaces between realities without losing any of them” (p. 379).
Clayton, Kymbra. (2005). Critiquing the Requirement of Oneness over Multiplicity: An Examination of Dissociative Identity (Disorder) in Five Clinical Texts. E-Journal of Applied Psychology. 1. 10.7790/ejap.v1i2.21.
—60
These types of symptoms are most responsive to psychotherapeutic and hypnotherapeutic interventions that target the DID alter system.
…
It is essential to educate the patient about the «shock absorber» effects of medications and not promise a «cure» from psychopharmacologic agents. This allows the patient to provide a much more realistic evaluation of the efficacy of the medications. The entire alternate personality system may be engaged in evaluating the efficacy of medications.
Loewenstein, Richard J. (2005) Psychopharmacologic Treatments for Dissociative Identity Disorder. Psychiatric Annals, 2005;35(8):666–673
—61
These wrong diagnoses then deny the patient the opportunity for an uncovering psychotherapy that would access and abreact their horrendous histories, repressed feelings, and tissue memories. The process of this type of psychotherapy facilitates internal understanding and leads to the breakdown of the amnestic barriers and ultimately to integration and unification of the multiple personality system. MPD is a hopeful diagnosis of a treatable condition and it is a privilege to be a witness, as a therapist, to this healing journey, especially with a patient who was chronically disabled and who becomes totally functional.
…
From a general sytems theory perspective, DID is not peculiar to the human psyche, because it is a mode of dyfunctional system organization that can occur in any system in the universe. The core features of DID, from a systems perspective, are the existence of abnormally dissociated subsystems that act as if they are not segments of the larger system, and which display radical failures of information transfer between subsystems. From this perspective, DID affects DSM-IV, federal governments, corporations, and many other systems. When subsystems fail accurately to differentiate self and other, and launch destructive attacks on other subsystems within human patients with DID, we call this DID. When the same thing occurs in the imnnme system, we call it an autoimmune disorder. The greater validity of DID is that it provides a window into dysfunctional systems of all kinds-insights from the psychotherapy of DID might be harnessed to yield isomorphic repair mechanisms for other dissociated systems.
Cohen, L. M., Berzoff, J., & Elin, M. R. (1995). Dissociative Identity Disorder: theoretical and treatment controversies.
—62
From the phenomenological perspective, the old model posited an alter system made up of only a f ew (usually no more than two or three) highly discrete, well-developed, alters in a stable configuration.
…
In the new MPD paradigm, the alter personality system is seen not as a static entity but rather as a creative, «structured process» (Kluft, personal communication, 1987) related to a variety of intrapsychic and defensive functions. In this view, the system of alters can be understood as having defensive, representational, and symbolic purposes, as well as being-in-the-world aspects.
Hence, sorne MPD patients may develop a relatively Iarge number of alters over developmental time and may preferentially use creation of new entities to handle many life issues, including additional trauma, object loss, the need for restitutive fantasies after being abused, and more or less conflict-free functions such as alters that handle work, handle parenting, perform specific tasks, etc. In this view, the whole system of self-states is seen as the «real» person.
—63
Disclosures and requests for help by one part of the system, without the agreement of other parts, are likely to generate internal civil war. This may be particularly intense if there is an idea that the therapist would favour fusion of personalities or abolition of certain troublesome personalities. This would be equivalent to an external agency taking sides in a conflict within a country.
One point that cannot be emphasised too highly is that for many patients a multiple personality system has been established as a means of surviving. To threaten this system may be experienced as a threat of death. In this way the therapist may be perceived as utterly dangerous, either through malevolence or ignorance. Nevertheless, the fact that the patient is presenting for treatment at all means that in some respects the system created for defence is breaking down, and this creates the motive for therapy.
—64
Even so, we did work fast and effectively. Introductions were made, fears were laid to rest and integration proceeded smoothly. While our relationship was brief and her final integration unusual (in that I was very new to her life and system), her story in many ways was not unusual at all. At the heart of it was a deep sense of shame. A shame of such monumental proportions that it must be hidden. Secrets of shameful events were guarded and kept under wraps.
…
Sometimes. Maybe. Yes. No. It all depends. : ) Everyone’s internal system is different. They might have some alters that are aware of some, but not all. Or all. Or none. It can be very complex. Or not. It all depends on the person.
Peterson Crawford, Leah. Not Otherwise Specified: a multiple life in one body, 15 year anniversary edition. (2017) Edición de Kindle.
—65
Throughout their lives, these women have had relational problems, but my clinical observation has been that there is a difference in the quality of the midlife relationships. The relational dilemmas occur internally within their systems of personality parts and externally within their social networks.
…
My clinical experience in working with dissociation indicates that each internal system has its own organization, and the components may or may not have a relationship with some or all of the other internal parts. The general pattern of organization for a DID system is basically similar for most people, but there is a unique twist to presentations of DID, which contributes to the difficulty of making an early accurate diagnosis.
…
This was not about integration as defined by the mental health professional or in the professional literature. The women were referring to a conscious connection, respect, and cooperation within themselves as it happened within their therapy and then generalized to other relationships. They chose to retain their internal systems, adjusting the internal relationships to maintain adaptive functioning in their lives.
Green, PhD, LCMHC, MA, NCC, DCC,, Elizabeth. Our Voices: Six Women With Multiple Personalities Talk About Life and Relationships in Their Midlife (2016) (pp. 44-45). Edición de Kindle.
—66
Some therapists of patients with DID tend to contact as many identities as possible to map the inner system of identities and to gain a sense of what to expect later in treatment.
…
The inner system of identities in adult DID patients seems to have a surprising degree of consistency from one patient to another: certain types of identities seem to be present in most patients with DID. Following a trauma, or more commonly a series of traumas, these different identities evolve to fulfill different functions within the system.
…
Within the system of identities, there may be one-way or twoway amnesias (compare Ellenberger 1970; Janet 1907). Identities tend to be grouped around certain themes or traumas. In very complex cases, there may be multiple systems of identities, with considerable amnesias between systems.
Bremner, J. D., & Marmar, C. R. (2002). Trauma, memory, and dissociation. American Psychiatric Pub.
—67
Part 3 is about using a whole system approach to the client, seeing parts of them as parts of the whole client that require help to move towards gradual integration. The key to this, the authors propose, is through recognising and embracing resistance in all its forms and working with this, so that the various phobias of inner experience, parts, memories, attachment and loss, and healthy change and risk-taking can be gradually faced.
…
CORE CONCEPT
The content of traumatic memories should not be ignored, but therapists should understand and work with the dynamics of the patient’s inner system and relationships when traumatic memories emerge or are avoided.…
A particular dissociative part must always be understood in the context of the person as a whole—the dynamic system of which the part is a subsystem. That is, it is important to grasp the functions of a given part within the whole person.
…
Organization of the Dynamic System of Dissociative Parts
Although each part may have some unique features on the surface, there are some typical underlying similarities in the basic functions of parts and in the way they are organized.
Treating Trauma-Related Dissociation: A practical, integrative approach (1st edn) (Norton Series on Interpersonal Neurobiology) Kathy Steele, Suzette Boon, Onno Van Der Hart W.W. Norton & Company, 2017). Reviewed by Louise Hamilton & Stuart Mitchell
—68
Análisis funcional de la fobia a las partes disociativas
El terapeuta debe haber hecho ya un análisis funcional inicial del sistema de la personalidad del paciente y sus diversos subsistemas (partes disociativas; véase el capítulo 11). La selección de las interventions apropiadas requiere un análisis funcional continuo de las relaciones dinámicas entre las partes disociativas dentro de la persona como un todo, de lo que inhibe o activa las partes disociativas, y de lo que ayudará a los sistemas de acción a volverse más coherentes y coordinados. La bibliografía sobre el TDI [trastorno disociativo de la identidad] a veces define este proceso como una “cartografía” del sistema de la personalidad del paciente (Fine, 1999; Kluft, 1999; Sachs & Peterson, 1996), lo que también puede aplicarse a la disociación estructural secundaria.
Van der Hart, O., Nijenhuis, E. R. S., Steele, K., van der Hart, O., & Ruiz, F. C. (2011). El yo atormentado: La disociación estructural y el tratamiento de la traumatización crónica. Desclée De Brouwer.
—69
With respect to his theoretical works on trauma and dissociation, Janet’s theory ofmultiple centers of consciousness can easily be extended to a theory of multiple self and multiple dissociated self-states as a condition of human life. Sullivan, on the other hand, even though he thought in terms of dissociated systems and did not discount the existence of multiple personality, conceptualized those dissociated systems as dissociated from one self-system.
…
These partially and wholly dissociated self states alternate and exert pressure on others to respond with the expected reciprocation, thereby perpetuating the same unhappy attitudes and distressing situations. Along the continuum, there is an increasing lack of integrity within the system of self states.
—70
But shame is more insidious. It’s not about what we did wrong. It’s about us being wrong, just because we are. It’s a core organising principle of our psyche, our identity and view of ourselves—‘This is who I am.’ Like a weed, it wraps itself around our entire system of selves, strangling our relationships, our good feelings, our experiences, our hopes. It can smother us to death.
…
When I did, they were reassuringly normal—people with careers, in relationships, with children, with the same sets of neuroses and anxieties as everyone else, but with this usually hidden, subset of experiences and the agony of trauma behind their eyes. Then there were others with DID where multiplicity was the central core of their daily existence, who spoke about ‘alters,’ ‘systems,’ and ‘fronting.’
Spring, Carolyn. (2016) Recovery is my best revenge: My experience of trauma, abuse and dissociative identity disorder (English Edition) (p. 77). Carolyn Spring Publishing. Edición de Kindle.
—71
According to this perspective, in the treatment of Sandy, all the “alters” were my patient(s). It followed that I would need to have a relationship with all of them, to the degree possible, and treat them as equals within the system. “They” would ultimately determine whether or to what extent integration would occur, not the therapist and the “host” personality. Putnam warns (1989), “Before a therapist performs a partial or final fusion, the therapist should try to determine whether the alters are ready for such a fusion” (p. 306).
—72
By shifting form a monolithic view of the individual— a view of him or her as a kind of black box— to a conception of the individual as comprised of multiple selves, a profound shift in one’s understanding takes place in which the framework of systems theory can be linked to the world inside the individual.
—
Sandra Watanabe (1986, and see her case study in this issue) is, as far as I know, the only family therapist who has systematically explored the implications of seeing individuals as comprised of multiple selves. She has developed an interesting model for working with what she calls our “internal cast of characters.” Her model represents the way that an experimental family therapist would conceive of and work with the multi-self system.
—73
Although the aim of the treatment was articulated by the therapist during the preparation for the table technique, it is helpful to again state that all of the ego states are part of the system and that the aim of the treatment is the elimination of the dissociative barriers and the facilitation of harmony and cooperation. The assumption is that self-states are listening and many are suspicious. Movies and many therapists have suggested that the aim of this type of treatment is the fusion of ego states into one cohesive state. One should assume that a realistic paranoia exists internally and should continually, throughout the treatment, remind the adult self (or any other self that is active) that ego states are not eliminated or “killed,” not even the most virulent and angry ones. Anger and hate should be explained to contain the energy and assertiveness that was channeled into defense. Borrowing from systems theory, the context and function of these self-states needs to be explained as having been adaptive at one time.
—74
The final approach in Fraser’s article addresses the issue of fusion or integration, a strong area of potential controversy for those diagnosed with or identifying as DID. Many individuals with DID strongly resist or oppose a psychiatrist or any other provider’s insistence that they integrate the various aspects of their personality into a cohesive whole. This process can feel disrespectful to the members of a system, and if you are reading this passage and have ever felt triggered at the suggestion that you need to integrate, you are not alone. In the following section where contributors speak to how their systems operate, you will read many insights around whether the word and concept of integration works (for two of our contributors it does), or whether other ways of looking at healing (e.g., cohesion, unity, community, diplomacy) are a better fit.
Marich, J. Pollack, J. (2023) Dissociation Made Simple: A Stigma-Free Guide to Embracing Your Dissociative Mind and Navigating Daily Life
—75
It is important to remember that the host, in a sense, is also an alter. We have found it clinically useful to reassure the host, and all of the alters, that they are all part of the same «person» or «system,» and that all parts have a role, function , and at one time or another have been a necessary part of the whole.
…
Repeated dissociation may result in a series of separate entities, or mental states, which may eventually take on identities of their own. These entities may become the internal «personality states» of a DID system. Changing between these states of consciousness is described as «switching.»
—76
When therapists began working with dissociative persons, the explicit goal was generally integration or fusion, a term that was used to mean fusing all the insiders into one person. This was usually conducted through a ceremony that joined the entire system or major parts, and was artificially induced by therapist-directed hypnosis. It often did not work, or created more problems than it solved.
As one example of how MPD can develop: During a cult ceremony, seven-year-old Shawn is locked in a cage with snakes, then physically tortured, and finally sexually abused. Shawn’s psyche can only take so much ( as can any of our psyches). So when Shawn is ready to snap, a new personality, a tougher personality in this case, is developed to handle the next wave of abuse. Or to handle the next scene-maybe of one of his parents sacrificing an infant or having sex with a neighbor.
Each time a new personality is developed, it becomes an inherent part of the host person’s system. Later in life, this can really cause some problems.
Ryder, D. F. (1992). Breaking the circle of satanic ritual abuse: recognizing and recovering from the hidden trauma.
—78
In trying to clarify the dynamics of personality dissociation one must remember that, despite their differences, basically all the schools of depth psychology agree that the ego, the personality, or the self is a highly complex entity comprised of systems and subsystems which, although in constant conflict in relation to separation and union, must work cooperatively if the individual is to make a satisfactory adaptation to the environment.
—79
Extraordinarily, an occasional individual comes apart functionally into two or more large portions of his original personality. These portions are not simple pieces but more or less automatic selections from the organized system which was the individual.
—80
The Alter Personality Systems
There were no significant differences between the males and females in frequency of types of alter personalities such as child, opposite sex, analgesic, depressed, opposite gender, alters reporting themselves as younger or older than the ehronologic age of the person, etc.
…
Overall, our clinical i npression is that Iliost of tins group of male patients showed less complex deyehrpment of alter personality systems than typical female patients. In addition, notable presentational differences among the alters such as wardrobe, accent, posture, etc. was less common among these male patients than among female MPI) patients previously studied by the authors.
—81
To understand DID, one must recognize that the mind of the DID individual is subjectively structured as a complex, dynamic, adaptive self-state system that, beginning in early childhood, evolves developmentally. Putnam (1997, 2016) conceptualizes the core phenomenology of DID as the state of multiple states, which can subjectively reconfigure in varying ways over time. Armstrong (2001) uses the simile of understanding light as both particles and waves. She conceptualizes DID both at the level of specific self states and simultaneously at the level of the dynamic self-state system. There is a third level of conceptualization: that of the “whole human being” across all states and the self-state system. For example, in the pharmacological treatment of DID, medications are unlikely to be effective unless the symptoms of a co-morbid disorder, e.g., a mood disorder, are experienced across the whole mind, not just in specific self states (International Society for the Study of Dissociation et al., 2011; Loewenstein, 1991b, 2005). In assessing behaviors in the DID individual, one must consider that a number of different self states, in coordination and/or in conflict, account for them, not a revolving door of independently acting “people.” In this regard, it is critical to focus on DID as a self-state system, not an assemblage of relatively independent, recurring entities with stable characteristics.
—82
The language is deliberately kept simple so that the younger members of your internal system can understand it.
…
Meeting your other selves can be frightening, exciting, painful and joyous. You may find some who you like a lot, others that scare you. You may have alters who are talented and sophisticated, others who are autistic, silent, or fragmented. You may discover alters who are destructive or who act in sexually inappropriate ways. You’re almost guaranteed to have children in your system, as well as protectors and persecutors.
—83
They were afraid to be known to me because of the fear that I might try to destroy them. I have heard of other cases where these parts became angry and punished the rest of the personality system.
…
However, it saves a great deal of time if you have already learned about these abuses and structured personality systems, so that your client does not have to teach you everything.
…
She did, however, permit me to ask the insiders in her personality system whether there was any memory regarding police.
Hoffman, W., & Miller, A. (2018). From the trenches: A Victim and Therapist Talk about Mind Control and Ritual Abuse. Routledge.
—84
In his recent book on the IF’S model, Schwartz (1995) explains his understanding of the developmental process of a healthy internal system:members of the system need time to discover their visions and preferred roles; to harmonize their relationships; and to balance influence, resources, responsibilities, and boundaries. The system’s leader also needs time to establish credibility, trust and a shared vision. If the system exists in a sustaining, nurturing environment during its development, this healthy state will unfold naturally and at its proper pace, which needs to be respected. (p. 135).
…
Together they form an internal family, which organizes in the same way as other human systems. Each part, in its non-extreme state, wants what is best for the internal system.
…
The goal is not to fuse all these personalities. Instead, the IFS therapist seeks to restore leadership, balance, and harmony in the internal system such that each part can take its preferred, valuable role.
—85
By understanding how the parts function in a DID system, where they’re more distinct and obvious, we’ll also be able to recognize the same functions in their more subtle forms as they occur in the rest of us.
…
When a DID patient starts therapy and begins to feel comfortable with the new therapist, the system will often begin to drop hints about its existence. If the therapist seems oblivious to those signs, the system will slip quietly back into the background, and the correct diagnosis will be missed. The system is also likely to go back into hiding if the therapist reacts with disapproval, alarm or excitement over a rare “curiosity.” (In my experience, the two most common mistakes therapists make with DID are recoiling in fear or becoming fascinated with the intricacy of the system.
—86
It appears that DID can be readily diagnosed in Scotland (Macilwain, 1992), Puerto Rico (Martinez-Taboas, 1989), and New Zealand (Altrocchi, 1992) by clinicians who inquire systematically for its features. DID personality systems I have treated in native North Americans have the same features as those described in the research literature.
…
The Personality System and the Inner World of the Personalities
Less compelling but far more crucial than their overt manifestations are their inner belief systems, cognitive processes, and complex interrelationships.
…
The alter personalities that reside in dissociative paracosms may also be likened to styles in art, in that they represent distinct patterns of behavior that are visually distinguishable by their characteristic communication techniques; some alters may also be identified by their function within the personality system.
…
Figure 2. A flower schema is used to represent the internal personality system, which is under attack.
—87
The set of alter personality states, usually referred to as the personality system, constitutes the personality of the individual. Most psychotherapeutic work is directed toward this larger personality system and thus toward the individual as a whole.
…
Additional alter personalities associated with life stresses, such as academic, athletic, social, or sexual challenges, may appear, and the personality system dynamics become more complicated and polarized.
…
First dissociative identity disorder presentations in older dissociative identity disorder patients frequiently involve a life event, such as the loss of a job, death of a parent, or a revictimization, such as a rape, that reactivates earlier conflicts and destabilizes the alter personality system.
…
Comfort with family treatment and systems theory is helpful in working with a patient who subjectively experiences himself or herself as a complex system of selves with alliances, family-like relationships, and intragroup conflict.
—88
Not only the inner systems that exist in persons with “DID” (dissociative identity disorder, formerly MPD) and “DDNOS” (a similar disorder, labeled “Dissociative disorder not otherwise specified”) but complex personality systems, intentionally structured into multi-layered hierarchies.
…
The currently favored theory of structural dissociation (Nijenhuis & Den Boer, 2009; van der Hart, Nijenhuis, & Steele, 2006), which more accurately describes the way personality systems operate, instead distinguishes between two kinds of states: the apparently normal personality, or ANP, and the emotional personality, or EP, both of which could include a number of parts.
…
In the first place, unlike the ANP, they are likely to recognize that they are part of a “personality system”. They may use the first person plural (“we”) when referring to that system.
Miller, A. (2018). Healing the unimaginable: Treating Ritual Abuse and Mind Control. Routledge.
—89
The point is that most multiples have personality systems with pockets of amnesia much of the time. And most multiples have personality systems at odds with themselves; they do not act in unison with all of their parts — that is almost definitional of a multiple.
Saks, E. R., & Behnke, S. H. (2000). Jekyll on trial: Multiple Personality Disorder and Criminal Law. NYU Press.
—90
In general, then, a child with potential and predisposition for dissociation may use that naturally occurring psychological mechanism to cope when exposed to overwhelming stress. If similar circumstances recur, the child’s dissociation may solidify into an alter personality system, especially if significant caretakers in that child’s life fail to relieve that stress or, worse, contribute to the continuation or recurrence of that stress.
…
The presenting personality may actively withhold information in order to protect the multiple personality system or because important personal material may just not be available to a given personality.
—91
Should additional trauma occur, and should the alter be unable to endure it herself, additional personalities may be created in order to take over for the overwhelmed alter. The host and alters are referred to collectively as the personality system.
…
A personality system can be large or small, but regardless of size, certain types of alters are typically present in DID clients.
Krakauer, S. Y. (2013). Treating dissociative identity Disorder: The Power of the Collective Heart. Routledge.
—92
How do we understand the role of an eating problem in the personality system of a patient with MPD? Some of the literature suggests that one or more alters tend to carry the eating problem (Levin & Spauster, 1992).
…
Therefore eating problems necessarily take many different forms, both among patients with MPD in general and within any one personality system (Goodwin & Attias, 1993).
…
Not one or two alters but a large part of the personality system sends its message with the aid of food and body image metaphors.
Bloom, C., Gitter, A., Gutwill, S., Kogel, L., & Zaphiropoulos, L. (1994). Eating problems: A Feminist Psychoanalytic Treatment Model. Basic Books.
—93
DISSOCIATIVE REACTIONS CONSIST OF THE SEPARATION OF ONE OR MORE components of the personality system from the rest.
…
Estrangement is one manifestation of the dissociative attempt to escape from excessive emotional tension and anxiety by creating a separation within the personality system.
Cameron, N. (1968). Personality development and psychopathology: A Dynamic Approach.
—94
Both of us, in written and verbal communication, made the staff psychologist and psychiatrist aware of her condition and asked them to look for evidence of the operation of her dissociative system. After six days of hospitalization, none of the hospital staff had talked to her or questioned her about her disorder. Instead, she was left completely on her own.
Martínez-Taboas, A. (1995). Multiple personality: An Hispanic perspective. Puente Publications.
—95
She offered children “a piece of white paper with a circle drawn on each side of it,” and invited them to draw their “outside head” and their “inside head.” Her goal is similar to that of Shirar: to help the child develop “a map of the internal dissociative system, by showing not only the parts but the kind of communication, or lack of communication, existing between them” (Baita, 2011, p. 61).
Malchiodi, C. A. (2008). Creative interventions and childhood trauma. In C. A. Malchiodi (Ed.), Creative interventions with traumatized children (pp. 3–21). Guilford Press.
—96
The dissociative system behaves in some ways like a group; a style of work which combines individual, group, family and organizational psychotherapy is required. By being receptive to the communications from various parts of the dissociative patient, the psychotherapist and the therapy setting become a focus of integration.
—97
More commonly, the alters appear to have some knowledge of each other, but some have a more complex awareness of the dissociative system than do others.
…
In many cases, the complex and bewildering nature of the dissociative system of alters argues against the possibility of iatrogenesis through suggestion or demand characteristics; the phenomena are often not what the therapist expects.
…
Their inner state of multiplicity is usually concealed, the outward display of differing alters being just the tip of the iceberg; most of the dissociative system is covert, actively concealed from the ‘public’. Revealing the system of alters to a therapist can feel like surrendering the security that has been depended upon throughout life so far, and can seem to raise the threat of annihilation.
Mollon, P. (1996). Multiple selves, multiple voices: Working with Trauma, Violation and Dissociation. John Wiley & Sons.
—98
A patient with a complex trauma history and a diagnosis of dissociative identity disorder (DID) had worked with the first author in stabilization efforts for about a year, with considerable gains in affect regulation, coping skills, and understanding of her dissociative system. Her self-system had gone from rather conflicted to far less conflicted, with her perpetrator introject permitting the therapeutic work.
…
It is of utmost importance that the therapist seeks to understand the entire dissociative system of the patient and to improve cooperation and communication among all parts.
—99
For example, it is common for the DID patient’s system of personalities to view the therapist as a savior, a perfect parent, a demanding disciplinarian, a harsh critic, a dangerous and devious enemy, and an incompetent and useless helper, among others.
…
Thus, even from the beginning of treatment, the therapist must encourage and reinforce the relationship of various personalities to the personality system as a whole (e.g., “I know you have the experience of just going away, but I want to encourage you to stay and feel painful feelings, or to try and stay close when other parts of you emerge.”).
Chu, J. A. (2011). Rebuilding shattered lives: Treating Complex PTSD and Dissociative Disorders. John Wiley & Sons.
—100
By regarding each part of the client as a survival resource and reframing even symptoms such as selfdestructive behavior as an attempt by parts to regulate or protect, the whole dissociative system and each part of it is validated.
…
You can guide clients to recognize the interconnectedness of their internal parts through understanding that the functional resources they each possess in some way serve the entire dissociative system.
Ogden, P., PhD, & Fisher, J., PhD. (2015). Sensorimotor Psychotherapy: Interventions For Trauma And Attachmnent. National Geographic Books.
—101
Second, the therapist should contract with the whole personality system so that each personality state is made responsible for what he or she individually says ; and does. It is also useful to find one personality state who can speak for the entire system.
…
An effort was made to find someone in the personality system who could inform the therapist about who was actually present in the system at the time.
Braun, B. G. (1986). Treatment of multiple personality disorder. American Psychiatric Pub.
—102
The development toward ever more clarity of the whole dissociative system also relates to the growing general power of action of patients and to the associated increasing integrative tendencies.
…
58. Individuals who consist of contrary needs and desires that they associate with a different phenomenal self, phenomenal umwelt, and phenomenal self-umwelt borders and couplings are dissociative systems. These individuals consist of a dissociative organism- environment system including plural phenomenal experiences and conceptions of self, umwelt, and relationships of this self and umwelt.
Nijenhuis, E. R. S. (2017). The Trinity of trauma: ignorance, fragility, and control: Enactive Trauma Therapy. Vandenhoeck and Ruprecht.
—103
During therapy, I have come to understand the workings of MPD and its effects on my life, and I have come to be grateful that I have been blessed with a personality system that allowed me to do graduate work and to make a place for myself in a college community.
…
My system had a simple start, but as I grew older, and as my world grew more complex, and as the number of physical and sexual encounters grew, my system grew more complicated.
…
After all, one member of my system is the screaming, writhing three-year-old who was twice pinned down at the hospital.
Phillips, J. (1996). The Magic Daughter: A Memoir of Living with Multiple Personality Disorder. Penguin Group USA.
—104
This picture presented the structure and complexity of her internal personality system in relation to Dissociative Identity Disorder. No one is outside of the hotel and the playground is empty, indicating that Marie would not reveal who she was. The lightning suggested an impending storm to ensure that the parts of her personality system remained indoors, and unseen.
Harden, J; Hill, M. Breaking the rules: Women in Prison and Feminist Therapy. (1998).
—105
Thereafter, history-gathering and exploring the system of alters and working with the issues of the individual alters take place. Only then is there a stage of metabolizing the traumatic antecedents of the condition.
…
This was not appreciated until therapy was well advanced, when it became apparent that “Bad William” often was involved in provoking fights in which Bill would have no chance to win, and would be hurt. For example, after one confrontation with mother over his dating, “Bad William” felt so guilty that he initiated a bar fight with several toughs, by whom he was thrashed. This describes only a fraction of Bill’s system of alters.
Ammerman, R. T., Hersen, M., & Sisson, L. (1994). Handbook of Aggressive and Destructive Behavior in Psychiatric Patients. New York : Plenum Press.
—106
Early in work with these alters, I mapped Carole’s system of alters. Some believe that mapping is suggestive and may create iatrogenic complexity, but therapists who are highly effective in treating DID regard mapping as a safety measure. By using mapping, therapists hope to learn what they are up against in terms of the structure and composition of the alter system to allow them to conduct a safer and more circumspect psychotherapy.
…
Once I was better informed about the personality system and spectrum of alleged abuses, I asked whether an alter(s) was willing to discuss and process its experiences.
Spitzer, R. L. (2006). DSM-IV-TR Case Book Vol.2: Experts tell how they treated their own patients. Washington, DC: American Psychiatric Pub
—107
Moreover, a multiple’s system of alters evolves over time, and sometimes it undergoes temporary integration and subsequent fundamental functional reorganization into a different system of alters.
…
A similar point works against the type CR principle, because a multiple’s system of alters at different times may divide along quite different functional lines.
Radden, J. (2004). The philosophy of Psychiatry: A Companion. Oxford University Press.
—108
Most people now being diagnosed with MPD have a number of alters, rather than just one, which are combined in what is conventionally called a ‘system’. There are endless variations: some make angry, aggressive alters to protect the children, or friends to alleviate the loneliness, or torturers who mimic the abusers. Some people have only child alters, but others go on making new personalities, which may be any age. Most MPD systems contain at least one member of the opposite sex. Some include animals.
…
Usually at least one member in a system is in some way disruptive, and the behaviour of alters — promiscuity, self-harm, addiction, aggression, phobias — is often what first brings people with MPD to the attention of a therapist. However, the crucial thing about the disorder, which distinguishes it from normal multiplicity, is not the nature and behaviour of the alters but the fact that they do not share a common memory. Although some personalities may share information there is always a communication ‘gap’ in an MPD system. The normal ‘household’, as multiple systems are sometimes called, is open-plan, while in people with MPD at least some of the personalities live in watertight compartments.
Carter, R. (2014). The people you are. Hachette UK.
—109
However, unless we concurrently understand MPD as an interactive system, we are at risk of destroying an adaptive construction without providing a useful replacement. We can lift the barriers to internal communication by hypnosis in order to retrieve encapsulated memories. We then flood the patient with a past she has well understood to be excruciating (Loewenstein, 1988). If, on the other hand, we understand how the MPD system works in its variety of levels, we can use the organization to support orderly change (Kluft, 1985).
…
The data that underlie my ideas about complex cognitive functioning in MPD come from the more than 50 such patients I have assessed as part of a research project on MPD at the Sheppard Pratt Hospital (Armstrong & Loewenstein, 1990). Because I invite the patients’ full self-system to enter into the assessment process, I have been able to observe the multi-leveled quality of their cognitive experience.
Sinnott, J. D., & Cavanaugh, J. C. (1991). Bridging paradigms: Positive Development in Adulthood and Cognitive Aging. Praeger.
—110
There is thus no hierarchically highest level dissociative part that guides lower level parts, which is an organization that can be described and understood in terms of nonlinear dynamic systems theory applied to human functioning.
…
Personality
Personality can be defined as a biopsychosocial system that determines an individual’s characteristic mental and behavioral actions (cf. Allport, 1961). This definition highlights the fact that personality includes perception and emotion; that perception, emotion, and thought involve mental actions, including decision making; and that behavior involves combined mental and motor action. Personality constitutes a whole system that has an ongoing tendency toward integration, that is, binding and differentiation of different components of experiences (e.g., perceptions, emotions, thoughts) as well as different experiences across time (Edelman & Tononi, 2000; Van der Hart et al., 2006). In dissociation in trauma, personality as a system includes two or more insufficiently integrated subsystems.
Ellert R. S. Nijenhuis PhD & Onno van der Hart PhD (2011) Dissociation in Trauma: A New Definition and Comparison with Previous Formulations, Journal of Trauma & Dissociation, 12:4, 416-445, DOI: 10.1080/15299732.2011.570592
—111
In the sessions described below, a severely dissociated young boy and his parents discover the dynamics underlying the child’s internal dissociative system. The therapist responded with attunement, respect and acceptance as together, they reached into the play space where the potential for attachment, repair and making meaning was waiting.
Sinason, Valerie; Potgieter Marks, Renée. (2021) Treating Children with Dissociative Disorders: Attachment, Trauma, Theory and Practice (p. 184). Taylor and Francis.
—112
The therapist must relate effectively to each of these internal fragments, seeking to improve the contribution of each fragment to overall functioning. The superordinate aim of integrative therapy is to promote the confluence of the entire system, not to strengthen dissociation between alters.
…
The internal helper alter is a useful ally in treatment and can serve as a consultant to the therapist, providing information about the total system. The ultimate aim of integrative therapy is to reverse the pervasive attachment disruption and splitting that have accompanied abuse.
…
Table 27-4. Stages in the integrative psychotherapy of dissociative identity disorder.
1. Establish a working alliance
2. Make the diagnosis, inform the patient, and mantain the therapeutic alliance.
3. Make contact with the different alters.
4. Explore the structure of the system of alters.
Ebert, M. H., Loosen, P. T., & Nurcombe, B. (2000). Current diagnosis & treatment in Psychiatry. New York : Lange Medical Books/McGraw-Hill
—113
The patient may be regarded as a system with its own rules of interaction. Here one learns the who, when, why, where, what, and how of the alters; their names (if any); age of onset and self-perceived age; the reasons for their creation and persistence; where they fit in the patient’s overall history and in their relationships within the world of the personalities; and their particular problems, functions, and concerns.
…
Such work should not be undertaken until one has some idea of the lay of the land in terms of the patient’s system of personalities and at least some intellectual insight into what material is likely to be encountered
Kaplan, H., Sadock, B. J., & Grebb, J. A. (1994). Kaplan and Sadock’s Synopsis of Psychiatry : Behavorial Sciences, Clinical Psychiatry. En Williams & Wilkins eBooks
—114
Tabla 2. Fases en los tratamientos de pacientes con MPD. Fases de tratamiento Objetivos y características Establecimiento de la terapia Diagnóstico y alianza terapéutica. Intervenciones iniciales Asegurar y estabilizar al paciente. Recopilación de la historia y sistemas de personalidades Centrada en reconocer los asuntos de cada personalidad y sobre todo, los patrones de interacción entre las mismas. Desarrollo Centrada en el modo de acción del suceso traumático. Tendencia a la integración-resolución Se priman los esfuerzos en la construcción de la comunicación, recuperación de material y las implicaciones de éste. Integración-resolución Reconciliación y cooperación entre las personalidades. Implicación en nuevos aprendizajes Nuevas estrategias de afrontamiento y consolidación de las mejoras. Control y seguimiento La hospitalización no suele ser necesaria
Romero-López, M. J. (2016). Una revisión de los trastornos disociativos; de la personalidad múltiple al estrés postraumático. Anales de Psicología / Annals of Psychology, 32(2), 448–456. https://doi.org/10.6018/analesps.32.2.218301
—115
alters. Within the personality structure of a person diagnosed with dissociative identity disorder (DID), the original identity of the person is seen as having been fractured into different “alters,” typically due to trauma at an early age. The alters typically have their own sense of history, emotions, and thoughts. The alter has a purpose within the dissociative system of the DID patient and that patient may or may not be aware (conscious) of the alter’s presence. Also known as “parts,” “fragments,” “identities,” “personalities,” “personality states,” “friends.” See DISSOCIATIVE IDENTITY DISORDER, MULTIPLE PERSONALITY DISORDER.
Corsini, R. J. (2002). The Dictionary of Psychology.
—116
More recently, clinicians experienced in treating patients with multiple personalities have questioned the ability of therapists to create entire personalities. They contrast the full-blown alternate personalities of true DID/MPD cases — personalities with wide ranges of affects and detailed life histories — with the kinds of stereotypic behavioral changes induced by hypnotic suggestion. However, it is not uncommon for new personalities to appear during therapy, personalities of which the therapist was initially unaware. Usually, in our own experience, these personalities preexisted therapy but chose to remain hidden. Often, a therapist encounters major players in the dissociative system months or even years after the onset of therapy. Furthermore, dissociation is a habit of mind, an
Lewis, M. (1996). Child and Adolescent Psychiatry: A Comprehensive Textbook. Lippincott Williams & Wilkins.
—117
Cada muñeca estaba «expuesta», lo que mi padre decía que significaba que no podía jugar hasta que el me dijera que era hora de que salieran del armario. Por la noche cuando me despertaba para abusar de mí, sacaba la muñeca de la personalidad que tenía que poner delante, o representar, con una personalidad de mi sistema interno de personalidades creadas. Cuando sacaba una muñeca del armario, decía, «Ya no está en el escaparate, ahora puede salir a jugar», y en aquella tierna edad, me gustaba cambiar la personalidad que mi padre elegía.
Taylor, B. (1999). Thanks for the Memories: The Truth Has Set Me Free!: the Memoirs of Bob Hope’s and Henry Kissinger’s Mind-controlled Slave : Used as a Presidential Sex Toy and Personal «mind-file» Computer (Gracias por los recuerdos).
—118
«No puedo controlar estos saltos (todo el cuerpo de la paciente experimenta una sacudida). He hecho de todo para que se quiten, pero cada vez es peor. Ahora los dejo estar, procuro hacer cosas relajantes (nueva sacudida) y esperar a que se pasen… Estoy desesperada.» En mucho casos, debajo de estos síntomas hay un sistema de partes disociativas que representan una alteración de identidad. En otros, pueden corresponder a bloqueos somáticos o a memorias preverbales.
Vázquez, A. G., & Barral, D. M. (2014). Trastorno límite de la personalidad y EMDR.
—119
Similarly, Kluft notes that clinicians need to focus on the content of a DID patient’s alter personality system and not the strict number of alters when examining complexity.66 For instance, he states that patients can replicate their system of alters during major life changes or stressors, thereby creating a «new and undamaged» version of the system and inactivating the previous system (a process termed «epochal division»).67 In one patient, the same system of alter personalities was replicated five times as the patient moved through different levels of schooling as well as during her divorce.68 Even though there were numerous alters present, the core active content of her system was still the original, smaller set of alters.69 However, in another case, a patient who was repeatedly abused for over ten years developed a different alter after every instance of abuse to avoid dealing with the trauma, leading to a highly complex system due to the diversity among the alters.70
Brennan, T.A. (2020). Determining medical decision-making capacity for patients with dissociative identity disorder: a patient-centered approach.
—120
The affected individuals may startle even with a sudden pat that could bring back many distressing and traumatic memories. Hence the family may require education regarding avoiding any unwanted touch. The affected individual should also have the liberty of autonomy to determine and reflect when inappropriate situations arise, with the alter and the affected individual being in denial. It helps the affected to understand the alters as their system.
…
Assessment of suicidality should consider relational aspects as well. Safety agreement may be helpful unless the overall condition points to an absolute potential for a suicide attempt. The latter may be due to the overall severity of the condition, suicidality claimed by the majority of host and alter personalities, severe major depression generalized to the whole personality system, or living in a highly abusive environment.
…
Experiencing Inside or Outside
Although mental intrusions from within (e.g., interference of alternate personality states) may have unlimited capacities to escape reality as an activity of the inner world, they are limited in agency. This is due to the partial control still maintained by the host and other personality states of the internal system.
Tohid, H., & Rutkofsky, I. H. (2024). Dissociative Identity Disorder: Treatment and Management. Springer Nature.
—121
Dissociation is defined as a failure in the process of integrating biopsychosocial components of experience within a unified personality system (American Psychiatric Association, 2013); dissociation can take place in, or affect, all areas or levels of psychobiological function (e.g., emotion, memory, identity, sensory perception, and motor control) (Indelli et al., 2018).
Hong Wang Fung, Chitat Chan & Colin A. Ross (2020) Clinical correlates of hearing voices among people seeking interventions for dissociation: a cross-cultural investigation, Psychosis, 12:4, 328-338, DOI: 10.1080/17522439.2020.1773910
—122
Although the first formulation is a more concrete way of thinking about experience, both are equally healthy and effective. In fact, many – perhaps most – individuals who resolve the problems that fueled their radical dissociative symptoms stop thinking of themselves as many people, even metaphorically. What was a necessary survival strategy — the complex and cumbersome system of self-states — gradually dissolves when it is no longer needed. Generally, this occurs with no instruction, suggestion, or assistance from the therapist.
Rivera, M. (1996). More alike than different: Treating Severely Dissociative Trauma Survivors. Heritage.
—123
The patient and therapist had come to the conclusion that there were several self-states who were sitting in the middle of the self-state system and “directing traffic,” stopping him from studying for his exams, sabotaging the treatment relationship, and undermining yet another treatment.
What I was met with was a system of self-states that was quite willing to reveal the architecture of the system as well as the frustration that existed because there were several adult self-states who, while on the surface cooperative, had regularly and secretly undermined the wish of other self-states to come to therapy and talk about their hurts.
Richard A. Chefetz (2017): Issues in Consultation for Treatments with Distressed Activated Abuser/Protector Self-States in Dissociative Identity Disorder, Journal of Trauma & Dissociation, DOI: 10.1080/15299732.2017.1295428
—124
If we want a testing that is representative of the DID patient’s full personality, we need to create a setting that encourages the participation of the patient’s full alter system. As in treatment, we can better appreciate and work with the “parts” if we have an understanding of the “whole.”
In most referrals for testing, the DID diagnosis is still open or the patient’s acceptance of alters is inconsistent. Therefore, I have found it best to encourage the involvement of all of the patient’s self-aspects in testing by framing my invitation of the divided personality system in everyday, normative terms.…
We can also encourage the natural coping of the self-system by asking the patient (“everyone”) for advice on how potentially dangerous or terrified alters can participate safely. Quite often, a DID patient has an alter who is expert at handling crises, and the patient can authorize us to call on this alter for help should it become necessary.
…
Initial stabilizations (contracting with specific alters and the personality system as a whole in order to control what were previously uncontrollable behaviors)
Spira, J. L. (1995). Treating dissociative identity Disorder.
—125
For sure, as the reader might remember, those early seeds of doubt sown when we began reading through my therapy notes ensured ongoing scrutiny and appropriate correction as therapy continued, the book progressed, and Cordelia’s understanding of her multiple personality system increased.
…
Victoria it seemed had in fact played a very vital role in keeping up appearances, and now, having revealed the cracks beneath the surface, the whole system appeared to be collapsing.
Hannah, C., & Discart, G. (2005). The Bluebell Children: Multiple personalities: The Art of Self-Deception. Athena PressPub Company.
—126
“I don’t want interference. Each alter does its part and stays there, protecting the whole system.” My lips pressed together. “I’m sorry. I’m not cooperating.”
Liston, S. (2017). My Altered Self: How God’s Gift of Multiple Personality Disorder Redeemed My Nightmare Childhood.
—127
Bruce accepted her in totality – meaning acknowledging and parenting each part that emerged over many years, demonstrating amazing insight and, particularly, without judgment. His display of a remarkable and uncanny ability to understand her complicated system of selves and to treat them with respect and caring, while acknowledging their unique needs, gave all parts of Dr. Bruch a chance to grow up – to develop within a nurturing relationship.
Bruch, D. (2016). Fractured mind: The Healing of a Person with Dissociative Identity Disorder. Createspace Independent Publishing Platform.
—128
Alters are also known as parts, alternate personalities, personalities, fragments, «headmates,» internal family members (such as «sisters,» «brothers,» «cousins,» and so on), or self-states. A system is the aggregate of all the changes in one body. Most, if not all, DID alters can take recurring executive control of the body in which they reside.
They may believe themselves to be of different age, gender, sexuality, appearance, source, or even species than the system’s actual body, and they may or may not be aware of these differences.
Moore, K., & Meyerson, M. (2023). Unveiling The Alters of Dissociative Identity Disorder: A Comprehensive Guide to Understanding, and Managing, Split Or Multiple Personality Disorder.
—129
BACKGROUND OF PATIENT
For six years, I have been working with a highly fragmented client with an extremely complex system, who reported severe abuse in a satanic cult over many years. She has a diagnosis of DID with approximately 300 child parts of self, making her a more extreme case of DID.
… As I described in my first paper (Shebini, 2019), I delivered Eye Movement Desensitization and Reprocessing (EMDR) therapy (Shapiro, 1995) with modifications for DID; the outcome was integration of approximately 100 parts within the personality system in a 12-month period.…
SESSION 3: PLANNED FUSION
Continuing with session 2 above, once the intensity of the memories became diminished, it was then opportunity to use EMDR. However, in this particular example, this was part C’s “last” remaining memory, so complete desensitization could have led to fusion, within the personality system.
Shebini, N. (2019). Flash Technique for Safe Desensitization of Memories and Fusion of Parts in DID: Modifications and Resourcing Strategies. Frontiers In The Psychotherapy Of Trauma And Dissociation, 3(1), 151-164. https://doi.org/10.46716/ftpd.2019.0031
—130
Her account of the polyfragmented system of personalities attests to the duration, frequency, and intensity of abuses that Jenny suffered. More than four hundred personalities have been documented in our therapy- This large number does not represent distinct persons in one body, but is shown to be Jenny’s experiences as responses to nearly unimaginable abuse.
…
For Jenny, for the whole system of personalities, great segments of time were lost to awareness, nearly two years, in fact.
Spencer, J. (2000). Suffer the Child.
—131
Turkus (1992) escribe acerca de la estabilización, mapeo del sistema de personalidades, reexaminación y reelaboración del trauma, y retomar la autovalía y el poder personal. Dentro de la literatura, también aparece de manera recurrente un énfasis sobre la importancia de la creación de límites firmes con pacientes con TID/TPM.
Schaefer, C. E. (2005). Terapia de juego con adultos.
—132
Peg, a 32-year-old factory worker, came to me in crisis in the course of treatment for MPD/DID with another therapist. She told me the following story, major elements of which, excluding the Satanic ritual segment, were corroborated by siblings. Peg had first discovered her system of more than 30 well-formed alters through handwriting differences in her therapy journal entries. But the therapy utilized aggressive hypnotic “recovery” tactics and was careening out of control.
…
The alters, a system of more than 30 people arranged in an intricate spatial topography, handled almost all of Peg’s relations with the world.
…
Her main alters methodically reorganized the topography of the system so that collaboration among her “people” was not hindered by structural barriers.
Krippner, S., & Powers, S. M. (1997). Broken images Broken selves: Dissociative narratives in clinical practice.
—133
The goal here is not integration or fusion of parts, but a cooperative engagement that benefits both the system as a whole and the individual components of the self. Therapists can offerclients reluctant to subscribe to this viewpoint an analogy of people riding together on a bus.
This metaphor graphically illustrates the futility of struggles for control amongst parts in the larger self system.…
One of the more striking aspects of this phenomenon is that it occurs without extensive or prolonged exploration of the parts comprising the client’s self system.
Gold, S. (2013). Not trauma alone: Therapy for Child Abuse Survivors in Family and Social Context. Routledge.
—134
Typically, there is a «host» personality who serves as the personality system’s ambassador to the interpersonal world, and a variety of alters who «come out” only at certain times or in response to particular events and stimuli.
…
The MPD system of alters generally seeks to avoid detection (Klult, 1985b), with fewer than 109 of true MPD cases presenting in a histrionic, florid manner which intentionally draws attention to the existence of alters.
…
In some MPD systems, animal alters will be found, as a result of the childhood fantasy creation of imaginary animal friends.
Bloch, J. P. (1991). Assessment and Treatment of Multiple Personality and Dissociative Disorders. Practitioner’s Resource Press.
—135
This arrangement served us all very well for several years, except for a couple of incidents when someone in the internal system felt an urgency to be out and in control of the body in order to express themself.
…
Maintaining my professional detachment, I was utterly fascinated—and at times horrified—by the capacity of my system to both split spontaneously and switch using Bompa’s techniques. Our journals captured the story unfolding in the Green Room. In the process, I learned some of my alters had also dissociated and had smaller parts.
…
I ever wanted to find peace, I had to listen to whatever my internal system brought forward. Back in the Green Room, there emerged the following description of the aftermath of the dining room science.
Armstrong, B. (2023). An apparently normal person
—
No surgió en Tumblr (ni TikTok), sino que existe desde de 1904
El lenguaje que decida usar un paciente es importante. Los alters no suelen querer llamarse a sí mismos «alters», al menos no al inicio. No es obligatorio tampoco llamar a la forma propia de funcionar un «sistema«. Es importante no forzar a una persona a usar un término con el que no se siente cómoda. Pero el término «sistema» no fue inventado en Tumblr (lanzado en el 2007, encontramos citas de 1904), sino que es usado por los autores más reconocidos de Trauma y Disociación en la actualidad y en el pasado.
Fotos y screenshots de algunos textos citados.
-

- Lanius. Neurobiology and Treatment of Traumatic Dissociation
-
- Vedat Sar. MD. Trauma and Dissociation in a Cross-Cultural Perspective
-
- Paul F. Dell. (2009) Dissociation and the Dissociative Disorders – 2
-
- Carter, R. (2008). Multiplicity the new science of personality, identity, and the self
-
- Mosquera, Dolores. (2019) Working with Voices and Dissociative Parts
-
- Sandra Wieland. Dissociation in Traumatized Children
-
- Fisher, Janina. Healing the Fragmented Selves of Trauma Survivors
-
- Hunter, Marlene E. Understanding Dissociative Disorders
-
- Yeung, David. Engaging Multiple Personalities. Volume 1
-
- Ross, Colin A. M.D. Treatment of Dissociative Identity Disorder
-
- Radden, J. (2004). The philosophy of Psychiatry A Companion
-
- Carvalho, Esly. Ph.D. Sanando la Pandilla que Vive Adentro
-
- Baita, Sandra. Rompecabezas.
-
- Michelson, L. K., & Ray, W. J. (2013). Handbook of Dissociation Theoretical, Empirical, and Clinical Perspectives
-
- ISSTD Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision. 2011 – 2
-
- Valerie Sinason. Attachment Trauma and Multiplicity
-
- Cohen, Barry M. Thayer Cox, Carol. Telling Without Talking
-
- Sadock, Sadock. Kaplan & Sadock’s comprehensive textbook of psychiatry eight edition
-
- Spitzer, R. L. (2006). DSM-IV-TR Case Book Vol.2 Experts tell how they treated their own patients
-
- Shapiro, R. (2016). Easy ego state interventions
-
- Giancarlo, T. J. Multiple personality disorder A challenge to practitioners
-
- Boon, SuzetteSteele, KathyVan der Hart, Onno. (2014) Vivir con disociación traumática
-
- Ammerman, R. T., Hersen, M., & Sisson, L. (1994). Handbook of Aggressive and Destructive Behavior in Psychiatric Patients
-
- Trujillo, Olga R. La Suma de mis partes
-
- Baer, Richard. Switching Time
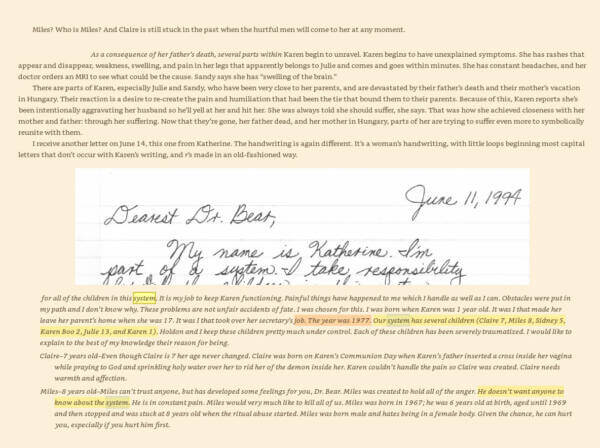
-
- Sinnott, J. D., & Cavanaugh, J. C. (1991). Bridging paradigms Positive Development in Adulthood and Cognitive Aging
-
- Schwartz, R., PhD. (2021). No bad parts
-
- James Chu. Rebuilding shattered lives
-
- Sinason Valerie, 2021. Treating Children with Dissociative Disorders
-
- Putnam, F. W. (1989). Diagnosis and treatment of multiple personality disorder
-
- Alderman, Tracy. Ph.D. Amongst Ourselves
-
- Boris Sidis, M.A. PhD. M.D. (Harvard) and Simon P. Goodhart, Ph.B.. (Yale) M.D. Multiple personality. An Experimental investigation into the nature of human individuality 1904
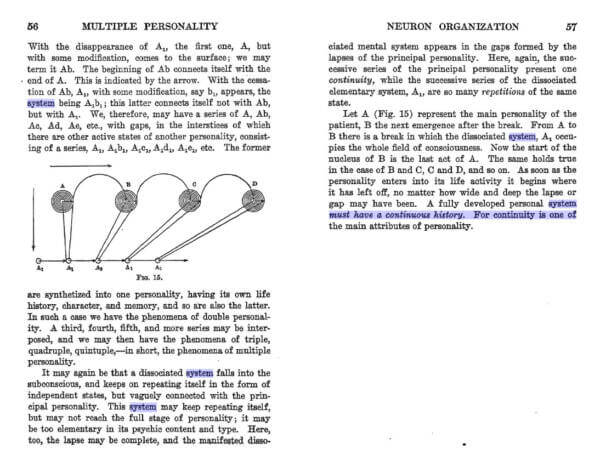
-
- ISSTD Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision. 2011
-
- Kluft, Richard P, M.D., Fine, Catherine G., Ph.D. Clinical Perspectives on Multiple Personality Disorder
-
- Fisher, Janina. Healing the Fragmented Selves of Trauma Survivors -2
-
- A.T.W.. Got Parts
-
- Mayer, Robert. Through Divided Minds
-
- Haddock, Deborah Bray. (2001) The Dissociative Identity Disorder Sourcebook – 2
-
- Ellert R. S. Nijenhuis PhD & Onno van der Hart PhD (2011) Dissociation in Trauma A New Definition and Comparison with Previous Formulations
-
- Haddock, Deborah Bray. (2001) The Dissociative Identity Disorder Sourcebook
-
- Paul F. Dell. (2009) Dissociation and the Dissociative Disorders
-
- Hunter. E. Marlene. MD. FCFP(C) Canadá. (2013) Manual Médico Para el Personal Cubano de La Salud Sobre Trastornos Disociativos
No es necesario usar el término sistema para uno mismo. Pero se usa en la comunidad científica.
La mayoría de personas con TID (sistemas, múltiples, plurales, personas que viven con TID, pacientes de disociación compleja, etc) pasamos la mayor parte de nuestros días en defensa del reconocimiento del TID como una condición real, que no te hace un asesino, que hay esperanza de tener una vida satisfactoria, que existen estudios, que mejora con un ambiente de comprensión y contención.
Creemos en la sana discusión científica y fundamentada, que tenga como prioridad mejorar el entendimiento, divulgar información correcta y humanizar las experiencias disociativas complejas.
Aclaraciones del diverso uso de «sistema» en el TID
Hay usos que significan diferentes cosas en esta visión sistémica. El enfoque de este artículo es su definición como conjunto de partes disociadas o alters.
Pero también puede significar un alter en sí mismo. Es decir, un alter es también un sistema de ideas (Morton Prince, 1906). Es por esto que en la Teoría de Disociación Estructural, cada parte disociada se le puede llamar un subsistema, es decir, un sistema (alter) dentro de un sistema más grande (persona total), quien a su vez crece en un sistema más grande (familia externa), que crece en un sistema más grande (ciudad).
Esto no se refiere a que un alter tiene varios alters, sino que, en general, cada identidad compleja es siempre un sistema de ideas. Pero a su vez, un mismo alter, en un TID complejo, puede también tener su propio sistema de alters, su propio subsistema. Imagínatelo como un fractal. Esa es la visión de la teoría de sistemas en general, cada sistema existe dentro de un sistema más grande, y es formado por sistemas más pequeños y elementales.
Así que, en todas estas referencias de este artículo, solo consideramos el uso del término «sistema» como el conjunto de partes disociadas, el total de partes, la persona en total.
Nota de edición: Hemos agregado más información desde la primera publicación de este artículo en 2020.



Gracias por la información y las referencias. Sobre todo me pareció excelente tu apego a la data científica, la educación, la discusión y corrección, esta clase de apertura y flexibilidad dialéctica suelen pasarse por alto y no está de más felicitar a quien expone estos valores. Excelente post!
Hola!! Me gusto mucho el contenido, disculpa tengo una duda a cerca de los nombres que cada sistema se pone, por ejemplo Long soul System. ¿Desde cuando en la historia cada sistema (Personita con TID) se pone un nombre particular para distinguirse?, ¿ quien lo implemento?, ¿cada sistema como lo elige?, ¿se los pone el mismo sistema o el terapeuta o psicólogo o psiquiatra se los pone ?. ¿lo eligen en terapia o se lo ponen cada sistema en particular?. Muchas Gracias de antemano ʕ•ᴥ•ʔ
Saludos!! Me pareció muy interesante y completo!